These simulations of BPPV treatment were created using a prototype of the BPPV Viewer in Amira software by Michael Teixido MD and Henri Traboulsi MD at The Delaware Biotechnology Institute of the University of Delaware. These simulations may be used for teaching purposes with attribution to these authors.
Posterior Canalithiasis
Diagnosis of Posterior Canalithiasis
The Dix-Hallpike maneuver is the workhorse for diagnosis of BPPV. In posterior canalithiasis, canaliths in the lowermost ear fall to the new lowest position causing an up beating and geotropic rotary nystagmus. This response can be interfered with by movement of other canalith masses if present, as seen below in the section on multiple canal BPPV.
Treatment of Posterior Canalithiasis
Brandt-Daroff exercises promote 90 degrees of movement around the posterior duct. When lying on the opposite side the posterior canal is parallel to the earth and no movement is provoked.
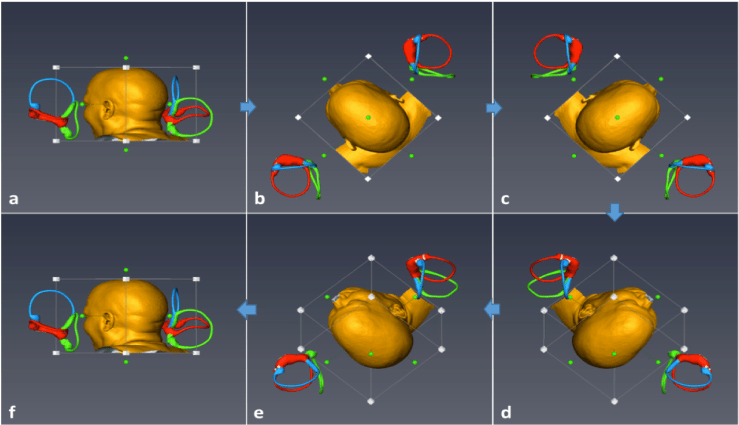
The Canalith Repositioning Procedure(CRP) or Epley Maneuver, is an effective way to remove canaliths from the posterior semicircular duct. The CRP shows how the corners of the room can be used to guide the 90 degree position changes needed for effective repositioning of otolith debris from the posterior canal to the utricle. The positions are 1,2,3 and sit up. When sitting up the head should be tilted forward to bring the common crus vertical, and prevent debris from falling back into the posterior canal. The maneuver should be repeated until no typical posterior canal response is seen. This may require 1-4 passes. When no response is seen, the patient rises by passing through the steps of the procedure one last time.
In patients with chronic disease and frequent recurrences in the same ear, the CRP can be done at home as a method of getting out of bed, and can be more time efficient than home Brandt-Daroff exercises.
180 Degree Displacement Maneuvers for Posterior Canalithiasis
Originally conceived as a treatment for posterior cupulolithiasis, the Liberatory maneuver works for posterior canalithiasis. Although not intuitive, it is sometimes easier to treat large patients with the Liberatory maneuver than with Canalith Repositioning. This is the only maneuver in the treatment of BPPV that needs to be done rather quickly to be effective. If the transfer is too slow the canaliths will fall back, rather than forward and over to the common crus. The Liberatory maneuver is only effective when the head is hung well below horizontal at both the beginning and the end of the transfer.
This treatment modification for posterior canal BPPV was developed in August 2006 by Dr. Teixido in the 3D visualization laboratory at the Delaware Biotechnology Institute. This exercise is appropriate for any BPPV patient, even if the side of disease is not known. The posterior canal exercise moves otoconia 60° farther around the circumference of the posterior semicircular duct with each repetition than conventional Brandt-Daroff exercises. The extra motion toward the posterior canal ampulla may enhance contact of the otoconia with dark cells at the base of the ampulla. Dark cells may play an important role in otoconia resorption. The exercise has 6 head positions, but is easy to teach.
360 Degree Displacement Maneuver for Posterior Canalithiasis
This variation of treatment is effective but only only possible with specialized, expensive and space occupying equipment. Observe closely and you can see there is a risk a conversion of posterior canalithiasis to anterior canalithiasis.
Lateral Canalithiasis
Diagnosis – Long Arm Lateral Canalithiasis
In most lateral canalithiasis otoliths are positioned in the intermediate segment of the lateral canal as shown here. This video shows bilateral lateral canalithiasis in order to demonstrate what happens in the upper most and lower most lateral canal in the Dix-Hallpike positions. In this video, the left Dix-Hallpike position is assumed first. In this initial position, little movement is provoked in the lower most lateral canal. Most nystagmus observed will come from the uppermost lateral canal. If this patient had only left lateral canalithiasis, it is possible no nystagmus would be observed until the right Dix-Hallpike position is reached. Lateral canalithiasis causes geotropic horizontal nystagmus in almost all cases.
Diagnosis – Short Arm Lateral Canalithiasis
In less than 10% of cases canaliths in the lateral canal are positioned in the anterior segment of the lateral canal. This causes an ageotropic horizontal nystagmus in the Dix-Hallpike position. This variation of lateral canalithiasis is called “ageotropic” lateral canalithiasis. In this video, right short arm canaliths may provoke ageotropic nystagmus when in the left Dix-Hallpike position.
In less than 10% of cases canaliths in the lateral canal are positioned in the anterior segment of the lateral canal. This causes an ageotropic horizontal nystagmus in the Dix-Hallpike position. This variation of lateral canalithiasis is called “ageotropic” lateral canalithiasis. In this video, right short arm canaliths provoke ageotropic nystagmus when in the right Dix-Hallpike position. When the patient continues to the left Dix-Hallpike position the canalith mass will move farther in the same direction and cause geotropic horizontal nystagmus. At this point the ageotropic canalithiasis has “converted” and typical geotropic horizontal nystagmus can be expected.
Supine Roll Test in Lateral Canalithiasis
The supine roll test is used to repeatedly provoke geotropic horizontal nystagmus in lateral canalithiasis. In accordance with Ewald’s Second Law horizontal nystagmus will be strongest in the direction of the affected canal. It is in this way that side of lateral canalithiasis is best determined.
The Supine Roll Test converts short arm to long arm lateral canalithiasis. When short arm (ageotropic) lateral canalithiasis is detected on Dix-Hallpike testing, the supine roll test will convert the short arm canalithiasis to typical long arm canalithiasis that has consistent geotropic horizontal nystagmus.
Treatment of Lateral Canalithiasis
Log Roll
The Log Roll (BBQ) maneuver is gold standard for treatment of lateral canalithiasis. The only requirement for success is knowing the side of disease. The maneuver displaces otoliths into the utricle where they can be absorbed by dark cells. The maneuver may be performed at home in patients with recurrent disease.
Performing the log roll in the wrong direction will create a case of short-arm “ageotropic” lateral canalithiasis. In this situation, the side of disease is confirmed and rolling in the opposite direction will help the patient.
Lateral canalithiasis can be a stubborn problem and require home treatment. A simple modification of Brandt-Daroff exercises can increase the effectiveness of the exercise in these patients. Rather than turning the head 45 degrees upward in each side-lying position, the patient looks forward at the wall. This increases otolith movement from 90 to 180 degrees. This increased angular movement increases their effectiveness.
Side Sleeping for Lateral Canalithiasis
Sleeping with the affected side up is an effective treatment for lateral canalithiasis.
The Gufoni maneuver is a short-cut of the log roll maneuver that is particularly useful in large patients who are difficult to roll. This video shows treatment of right lateral canalithiasis. The patient moves to the left lateral position with the affected side up, then after a pause turns the face to the floor. After another pause the patient sits up.
Anterior Canalithiasis
Diagnosis of Anterior Canalithiasis
The diagnosis of anterior canalithiasis can be difficult. Because of the position of the rotation axis of the superior canal through the eye, mostly downbeating nystagmus is seen. The rotatory component can be difficult to see. If the dix- hallpike is performed to horizontal as seen above, no movement will be provoked in the uppermost canal. This fact can be used to separate anterior from posterior canal responses in multiple canal BPPV.
With the head hanging Dix-Hallpike maneuver, anterior canaliths in the uppermost anterior canal will move causing downbeat and rotary nystagmus. It should be noted that in this head hanging position canaliths in the lowermost anterior canal will also move. This is important because there is an inaccurate general impression that only canaliths in the uppermost anterior canal move.
Treatment of Anterior Canalithiasis
Perhaps the most simple treatment of anterior canalithiasis is the CRP. The left CRP works for left anterior canalithiasis and the right CRP work for right anterior canalithiasis. Below are a series of images that demonstrate the effectiveness of the standard CRP for anterior canalithiasis. Note that there is no otolith progress in position 3 because the anterior canal is parallel to the earth in this position.
A short-cut “reverse-Epley” has been described for anterior canalithiasis. It treats the uppermost anterior canal and also works:
In Left anterior canalithiasis the Right Dix-Hallpike position is assumed. The patient moves from CRP position 1, to position 3, pauses, then sits up.
A left to right Epley maneuver for right anterior canalithiasis does not work:
Unrecognized anterior canalithiasis treated with a standard Epley maneuver can cause confusing eye movements, and will not effectively reposition anterior canaliths.
The Casani Maneuver is perhaps the most simple way to treat anterior canalithiasis. The maneuver works regardless of which anterior canal is affected.
With special repositioning equipment, anterior canaliths can be repositioned with a 360 degree head over toes rotation.
Brandt-Daroff exercises are not effective in treating anterior canalithiasis.
Deep Brandt-Daroff Exercises, proposed by Dr. Michael Teixido for home treatment of anterior canalithiasis, can be used in patients who cannot hang the head sufficiently to perform the Casani Maneuver. Deep Brandt-Daroff exercises require the patient to hang the head below horizontal in each lateral position.
Multiple Canal BPPV
Simultaneous canal involvement is a diagnostic challenge. Traditional Dix-Hallpike testing to the head hanging position can provoke canalith movement in every canal. Initial testing to horizontal, followed by head hanging, can separate responses from posterior and anterior canals.
An Expanded Dix-Hallpike Maneuver has been proposed by Dr. Michael Teixido and has proven efficient in the clinic on all patients, and effective in separating responses from the posterior and anterior canals. Note that there is no need to sit the patient up between the right and left positions in this 6-part maneuver.